|
Source : Journal of Endourology Volume: 18 Number: 1 Page: 7 -- 16 DOI : 10.1089/089277904322836596 Publisher : Mary Ann Liebert, Inc. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ABSTRACT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Journal of EndoUrology Volume 18 Number 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Purpose: To perform in vitro and in vivo tests using a clinical lithotripter in order to determine whether a bifocal reflector is more efficient and produces the same or less tissue damage than a conventional ellipsoidal reflector for electrohydraulic lithotripters. Materials and Methods: A standard ellipsoidal and a novel bifocal reflector were tested on a Tripter Compact lithotripter (Direx Medical Systems, Petach Tikva, Israel). The bifocal reflector was constructed by joining two sectors of two rotationally symmetrical ellipsoidal reflectors having different distances between their foci. The F1 foci of the sectors coincided, creating a separation between the F2 foci. The fragmentation efficiency of the reflectors was compared using kidney-stone models. Shockwave-induced trauma was evaluated in vivo by treating both kidneys of six healthy dogs. One kidney was exposed to shockwaves generated with the conventional reflector, and the other kidney was treated using the bifocal reflector. Pressure measurements were obtained for both reflectors using needle hydrophones. Results: The new design appeared to be more efficient than the conventional reflector in breaking up kidney-stone models. Tissue damage did not increase when using the bifocal reflector. Conclusion: The use of bifocal, instead of standard ellipsoidal, reflectors should be considered as an alternative to improve extracorporeal shockwave lithotripsy. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Dr. R. Munoz Montastruc * Dr. P.P.Tirolien |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Material Methods :
MATERIAL AND METHODS: Between March 2000 and July 2002, we had separated two groups of patients with lower calyx lithiasis (100 each group).The treatments had been done with a NovaUltima lithotripter of fluoroscopic and ultrasound scan (Direx). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Florida on February 11, 2003 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| By: Dr. Cosentino of Sienna |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ESWT IN THE TREATMENT OF INFERIOR CALCANEAL ENTHESOPHYTOSIS: PREDICTION OF OUTCOME BY FAN-BEAM DUAL-X-RAY ABSORPTIOMETRY (D.X.A.). The purpose of our study has been to evaluate variation in the density of enthesophytosis associated with the clinical outcome after ESWT. Painful heel is a common syndrome with evidence of an inferior calcaneal enthesophytosis in about 50% of cases. The patients feel severe pain in the inferior aspect of the heel, especially in the morning and after a period of rest. The condition is slowly progressive to the extent that the patient may become disabled. The cause of this clinical entity remains enigmatic and is not clear. However, numerous factors have been claimed: functional overuse, degenerative diseases, inflammatory diseases and metabolic diseases. The conservative methods of treatment usually adopted included: insole supports, injections of local anesthesia and corticoids, antiphlogistic medication. 20 patients (14 females and 6 males) were examined aged between 40 and 70 years, with a mean age of 53 years, showing talalgia associated with enthesophytosis of the plantar fascia. Inclusion criteria were: pain over the radiologically examined heel spur and unsuccessful conservative therapy (insole supports, injections of local anesthesia and corticoids, analgesics and non steroidal anti-inflammatory drugs) during the 6 months before referral to our hospital. The exclusion criteria were: arthritis (rheumatoid arthritis, spondylartritis, crystal induced artropaty), neurologic abnormalities, nerve entrapment syndrome, pregnancy, age under 18 years, infectious or tumorous diseases, ulcerations, bursitis. No other treatment or drug was used during the 4 weeks before the trials began or during the study period. During the periods of treatment and follow-up only the use of insole supports were permitted. All patients were informed of and consented to the treatment methods. A ESWT system was utilized Orthima by Direx Medical Systems Ltd. That is characterized by an electrohydraulic shock wave source assembled on a mobile arm with full possibility of movement. It is also equipped with a sonographic system with Linear Array and 7.5 MHz probe. The therapy comprised 5 treatment (1 every 7 days), each treatment consisting of 1200 shocks with a frequency of 120 shocks per minute, the energy density utilized varied from 0.03 mj/mm to 0.4 mj/mm. Since pain could use high energy mostly during the first treatment, all patients during the first treatment, were treated with an energy density of 0.03 mj/mm for the first five minutes, which was the progressive increasing of up to0.28 mj/mm. During the second treatment, all patients were treated with an energy density of 0.28 mj/mm for the first five minutes, which was the progressive increasing of up to 0.4 mj/mm. During the other treatments the energy density was 0.4 mj/mm. The shocks were aimed at the enthesophytosis that was identified during sonographic examination. Local anesthetics were not used during the procedure. Pain level were evaluated by Visual analog Scale (VAS), ranging from 0-no pain to 10-maximum pain, at rest, following walking and after normal daily activity. Such assessment was made before, at the end of the therapy, after 3 months and after 6 months. Variations in the density of enthesophytosis were evaluated by dual-x-ray absorptiometry (DXA) at baseline and after 1 month from the end of therapy. Bone Mineral Density (BMD) and Bone Expert version 1.72; in each patient was created a region of interest (R.O.I.) to include the enthesophytosis and to exclude the os-calcis cortex. This R.O.I. remained unchanged for lateral controls. The non parametric Wilcoxon-test for dependent samples was applied to compare means of VAS, the paired Student T-test was applied to compare changes in BMD and BMC. A significant decrease of VAS (P<0.0001) was observed just after the treatment and after 3 and after 6 months at the three reference points of at rest, following walking on awakening and after normal daily activity. Densitometric analysis of enthesophytosis showed a significant decrease of bone mineral content (BMC) (P<0.001) and a significant increase of bone mineral density (BMD) (P<0.0001) after 1 month from the end of the therapy. In this study we did not observe side effect of ESWT< such as consecutive bleeding, superficial or deep hematoma, or clinical signs of nerve lesion. A temporary, slight redness of the skin and a transient increase in pain levels are within the norm. Our results showed that ESWT has a safe and efficacious effect on the painful symptomatology and that the improvement in painful symptomatology can be correlated with a decrease of BMC of the enthesophytosis. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Institution: Institute of Rheumatology, Policlinico Le Scotte Viale Bracci |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Objective : The aim of our study was to evaluate the clinical and radiological response of chronic calcific tendinitis of the shoulder to extracorporeal shock wave therapy (ESWT) in single-blind study. Methods : 70 patients were examined, showing chronic, symptomatic, calcifying tendinitis of the shoulder. A single-blind randomised study was performed with 35 patients undergoing a regular treatment (group 1) and 35 a simulated one (group 2). A ESWT system was utilised "Orthima" by Direx Medical System Ltd. Pain and functional assessment was carried out according to Constant and Murley. Variations in the dimension of the calcification was evaluated by anteroposterior x-ray films. Results : A significant decrease of pain and a significant increase in shoulder function was observed in group 1. Examination by X-ray showed partial resorption of the calcium deposit in 40% of cases and complete resorption in 31% of cases in group 1. In the control group no significant decrease of pain and no significant increase in shoulder function was observed. No modification was observed by X-ray. Conclusion : Because of its good tolerance, safety, and clinical radiologic response, ESWT should be considered as alternative therapy for chronic calcific tendinitis of the shoulder. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Author: Mauro Meyer |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Introduction : Trochanteric bursitis is the inflamation of the trochanteric bursa causing chronic pain on the lateral aspect of the hip and tight, irradiating to the knee; more frequent in women more than 40 years and less than 60 years. The current treatment consist of non-steroidal anti-inflamatory agents, physiotherapy(ultrasound and similars) and local injection of steroids with or without anaesthetic drugs. When these conservative procedures fail, the option is the surgical treatment. We used the shockwave therapy for the treatment of the trochanteric bursitis after the fail of the conservative procedures and before the surgery like a last effort to avoid it. Material and Methods : 18 patients, all women aging from 40 to 86 years (media 60), with chronic trochanteric bursitis for more than 12 months, having done all the conservative procedures without success, were submited to shockwaves therapy between march and july 2001. The diagnoses was confirmed by clinical examination plus a thickening of the bursa wall by echography or irregularieties or peritrochanteric calcifications on x-rays. By palpation, the points of pain were localized in the region of the great trochanter and was apllied 600 shockwaves per point of pain, resulting in 1500 shockwaves if it was just one point up to 3000 shockwaves if were more than one point. Patients helped in the depth location of the impact, and no analgesic or sedative were used before, during or after the treatment. Pressure waves were applied using the Orthima of Direx Medical Systems. The energy used vary from level 1(0,03mJ/msquare) to 3(0,2mJ/msquare). In september 2001, all patients were revised and asked about the pain in a Visual Analogue Scale (VAS) of 10, and asked about satisfaction or not about the result of the treatment. In october 2001, patients not satisfied with the result of the treatment were invited to do more one session, and one patient did not accept repeat the treatment. Patients satisfied but with VAS level less than 8 were invited to do the same, and all accepted repeat the treatment. Results : 3 patients were unsatisfied with the treatment and the other fiftheen were satisfied. The results with the VAS vary from 5 to 10 in the satisfied group and zero for all patients in the unsatisfied group. 2 of 6 patients that used low energy level 1 were from the unsatisfied group and the others four of the satisfied group were two in level 5, one in level 8 and one in level 9 in the VAS. The results of the new treatment of the patients of the usatisfied group and of the satisfied group with VAS level less than 8 will be shown in the congress. Conclusions : Patients may know very well about the possibilities of the treatment and agree with the perspective of more than one procedure. Probably, becouse is a large area to be treated, it is difficult to solve it just in one procedure in some patients. It is important show to the patients the difference of the pain from the trochanteric bursitis and from other pathologies like low back pain, becouse when they can differentiate it, the sactisfaction with the treatment were almost 100%. Shockwave therapy for treatment of trochanteric bursitis seems to be a new and efficient treatment reducing dramatically the number of patients that go to the surgery. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Institution: Istituto di Radiologia Dell'Universita' Degli Studi del Piemonte Orientale "Amedeo Avogadro", Facolta' di Medicina e Chirurgia di Novara |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Purpose : Since July 1999 we conduced an experience in the treatment of the tendinous pathology, using a portable shock-wave lithotriptor, designed for low energy. It's a non-invasive treatment without the aid of local anestetic (in the majority of cases). Material and Methods : We examinated 142 patients (85 males and 57 females, average 52.5 years) in the period from July 1999 to March 2002 using the "Orthima" lithotriptor marketed by "Direx Medical Systems". This is a lithotriptor of electro-hydraulic type. The pulsation frequency is 120 pulses/minute and the energy supplied can vary from 0.0003 up to 0.5 mj/mm2 with a maximum penetration capacity up to 65 mm. In all cases a preliminary diagnostic examination was carried out (RX or, when necessary, US and/or NMR). From January 2002, before and after each treatment, we've used a clinical evaluation forms. Each treatment includes a series of sessions varying, cases by cases, between 5 and 10 with intervals of 3-5 days, depending on the clinical progress and the type of pathology. Results : The target was pain absence-reduction. We obtained satisfying results in 68% (97 patients) of cases and lack of success in 31% (45 cases) of the patients treated. Conclusions : Keeping in mind the repeatability of the therapeutic cycles, usually well tolerated by the patients, we also believe that low-energy shock waves therapy represent an important alternative to other conservative anthalgic treatments for common people and particularly for athletes. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1) Introduction A .." Unfortunately current lithotriptor designs have not been based on fundamental advances in the basic science of SWL vis-?-vis stone comminution and tissue effects. The result has been that newer generation machines have not improved outcomes for patients and indeed may be both less effective in breaking stones and more traumatic to renal tissue. "
2) Page 9 3) Page 10 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Brian Saltzman MD. Beth Israel-Deaconess Medical Center |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ABSTRACT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
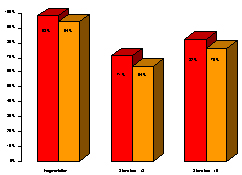
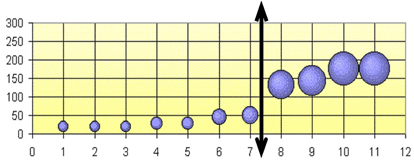
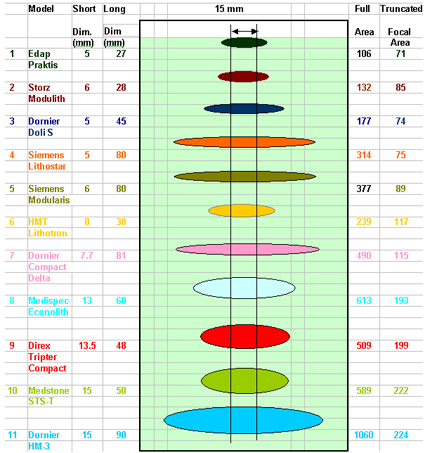
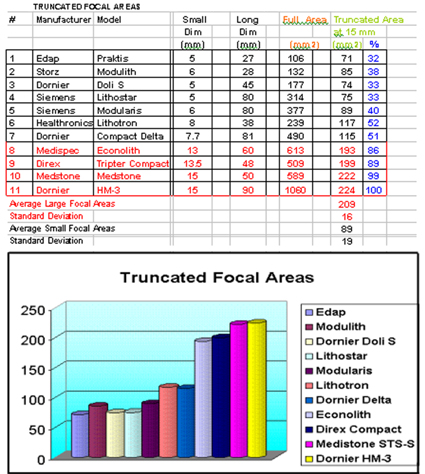
The Peak Pressure at F2 and the Focal Area are the traditional parameters used to compare the performance and effectiveness of the Shock Wave produced by different lithotripters. Lately, new electromagnetic lithotripters were introduced, some with higher Focal Peak Pressure. This fact may lead to believe that they are more efficient than the traditional spark gap systems. At the same time all electromagnetic systems have very thin focal areas, much smaller than the typical stone size, and therefore the available energy is not optimized for stone fragmentation, usually requiring much more shocks compared to a traditional Electrohydraulic lithotripter. The Focal Cross Section at F2, the Truncated Focal Area and Volume are 3 new tools which allow a more accurate evaluation of the Shock Wave characteristics and efficiency of different lithotripters. Eleven currently used lithotripters including the Dornier HM-3 were compared: The results show two categories of Lithotripters: a) Large Focus: Dornier HM-3, Medstone STS-T, Direx Tripter Compact and Medispec Econolith. b) Small Focus: All electromagnetic lithotripters, plus Edap Praktis and the Healthronics Lithotron. The Average Focal Cross Section for Large Focus lithotripters is 5 times bigger than the small ones. The Average Truncated Area is 2.35 times bigger and the Average Truncated Volume is 5 times bigger in Big Focus Lithotripters compared to Small Focus ones. This may help to explain why usually the electromagnetic lithotripters require much more shocks to break stones and have larger retreatment rates. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| INTRODUCTION | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Various lithotripters using different Shock Wave technologies are currently offered to treat stones in the urinary tract. In order to compare the various systems offered, Urologists analyze their technical specifications to evaluate their performance. (Ref 1) Traditionally the Peak Bar Pressure at F2 is the first parameter considered as an indicator of the available energy of a lithotripter and, therefore, has served as a first indicator of the efficiency of the system. Some confusion existed in the past regarding the numerical value of this Pressure at F2. Due to specific conditions of the Shock Waves, the measurements done with the older Piezoelectric Crystal sensors lead to erroneous high values of pressure (above thousand bars). During the last years a new precise sensor made of a membrane of Poly Vinyl Duo Fluoride (PVDF) was developed and adopted by FDA as the only one to be used in Pressure measurements (Ref 2). Using PVDF, the pressure values recorded are "smaller" compared to old Piezoelectric Crystal sensors, but obviously this is are more accurate and "real" values. Recently, new Electromagnetic lithotripters were introduced some of them with higher Peak Bar Pressure. This fact leads one to believe that they are more efficient than the traditional spark gap systems. Looking carefully we can see that this may be misleading. A correct analysis requires one to look not only at the Peak Bar pressure but also at the focal area geometric dimensions. All Electromagnetic systems have very thin focal areas - much smaller than the typical stone size-and, therefore the available energy is not optimized for stone fragmentation. The Total Focal Area which is also used sometimes to compare different lithotripters may be misleading too, because it does not take into account the fact that the typical stone size is much smaller than the long axis of the Focal ellipse and therefore a big portion of the energy is not applied to the stone. In order to clarify this issue three new tools were developed and are presented: b) The Truncated Ellipse Focal Area c) The Truncated Focal Volume. They will allow a more precise geometrical comparison of the Focal Areas of different lithotripters and hence their effectiveness. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MATERIALS AND METHODS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
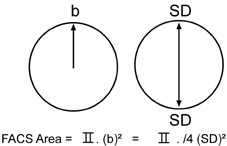
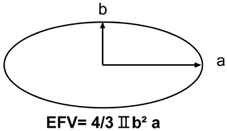
1) Focal Area Cross Section (FACS) The easiest way of visualizing how much of the stone is subjected to pressure is to look at the Cross Section of the ellipsoid at F2 (Like "cutting" the ellipsoid/cigar at F2 and looking at the circle that originated).
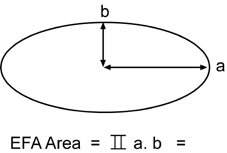
b = Focal Short Radius =SD/2 2) Ellipse shape geometric function 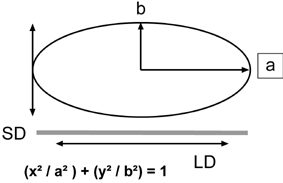
Using the ellipse Long Radius a , and the Short Radius b, we can calculate the full Ellipse area using the formula
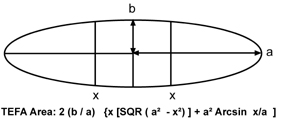
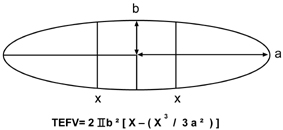
4) Truncated Ellipse Focal Area (TEFA)
RESULTS
2) The Truncated Ellipse Focal Area The Graph below represents all focal ellipses and their truncation.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DISCUSSION | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This may explain why the electromagnetic devices typically require significantly more shocks to adequately fragment kidney stones and also may result in higher retreatment rates. Recently, concerns have been raised ( Ref 5) regarding the fact that some new Electromagnetic Lithotripters that have very small focal areas and extremely high peak positive pressures are reporting higher clinically significant hematoma rates of 3 to 12% (Ref 6,7 and 8). A trend that is worrisome. It is becoming clear that the electromagnetic devices with very long and thin focal area/volumes are not suited to fragment stones. The Truncated Areas and Volumes are intended to advance the discussion relative to the effectiveness of various lithotripters. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| REFERENCES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. J. Stuart Wolf, Jr. M.D. Issues in choosing a Lithotriptor: Concepts in Design and use. AUA, 2001. 2. Lewin P.A. and Schafer M.E. "Shock Wave sensors: Requirements and Design. J. Lithotripsy and Stone Disease vol. 3 pp 3-17, 1991. 3. IEC International Standard pressure Pulse Lithotripters-Characteristics of Fields. 1998 -04 Annex C, page 21. 4. FDA Guidance for the Content of Premarket Notifications (510 k) for Extracorporeal Shock Wave Lithotripters Indicated for the Fragmentation of Kidney and Ureteral Calculi. August 9, 2000. Page 6. 5. 1st International Consultation on Stone Disease Committee 8: Bioeffects and Physical Mechanisms of SW Effects in SWL. Chairman: James E. Lingeman, M.D. et al. 6. Kohrmann KU, Rassweiler JJ, Manning M, et al. The clinical introduction of a third generation lithotriptor Modulith SL 20. Journal of Urology, 1995; 153:1379-1383. 7. Stefan T, Thorsten B, Chaussy C. Reduced retreatment rate by anatomy related shockwave (SW) energy. Journal of Urology, 1998; 159:S34 (abstract). 8. Piper NY, Dalrymple N, Bishoff JT. Incidence of renal hematoma formation after ESWL using the new Dornier Doli-S lithotriptor. Journal of Urology, 2001; 165:S377 (abstract). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
100 treated cases with NOVA ULTIMA Extra Corporal Lithotripter Dr. Ruben Munoz, Dr. Pierre P. Tirolien |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
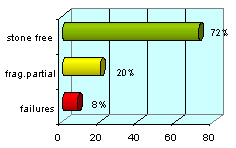
The lateral posture permits an excellent ultrasound scans image avoiding abdominal and suprarenal folds and also an improvement to the skin contact with the membrane. Results: The results in a three months period had been:
The best results obtained were with the pelvic and lumbar urethral stones (82%)
Discussion: For the kidney and urethral stones treatment on obese patients the lithotripter features are very important and the operator experience too. The knowledge and application of the localization systems permits to the specialist to obtain a better percentage of stone free. These techniques are important for these patients due to the posture on the table, which is fundamental to obtain a good result (50% in lateral posture with ultrasound scan). Conclusion: The indication of using ESWL on obese patients is a good choice but we always have to be respectful with the criteria of selection. The percentage of stone free in a three-month period has been satisfactory and the complications are similar to the ones published by other authors.
XIV National Conference of Lithiasis and Urinary Endoscopy,
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||