|
Source : Journal of Endourology Volume: 18 Number: 1 Page: 7 -- 16 DOI : 10.1089/089277904322836596 Publisher : Mary Ann Liebert, Inc. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ABSTRACT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Journal of EndoUrology Volume 18 Number 1 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Purpose: To perform in vitro and in vivo tests using a clinical lithotripter in order to determine whether a bifocal reflector is more efficient and produces the same or less tissue damage than a conventional ellipsoidal reflector for electrohydraulic lithotripters. Materials and Methods: A standard ellipsoidal and a novel bifocal reflector were tested on a Tripter Compact lithotripter (Direx Medical Systems, Petach Tikva, Israel). The bifocal reflector was constructed by joining two sectors of two rotationally symmetrical ellipsoidal reflectors having different distances between their foci. The F1 foci of the sectors coincided, creating a separation between the F2 foci. The fragmentation efficiency of the reflectors was compared using kidney-stone models. Shockwave-induced trauma was evaluated in vivo by treating both kidneys of six healthy dogs. One kidney was exposed to shockwaves generated with the conventional reflector, and the other kidney was treated using the bifocal reflector. Pressure measurements were obtained for both reflectors using needle hydrophones. Results: The new design appeared to be more efficient than the conventional reflector in breaking up kidney-stone models. Tissue damage did not increase when using the bifocal reflector. Conclusion: The use of bifocal, instead of standard ellipsoidal, reflectors should be considered as an alternative to improve extracorporeal shockwave lithotripsy. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Brian Saltzman MD. Beth Israel-Deaconess Medical Center |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ABSTRACT | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
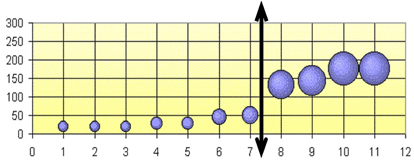
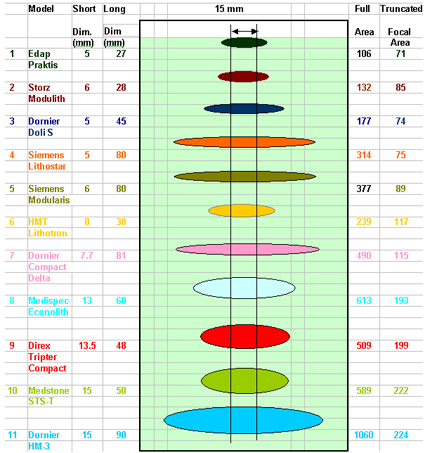
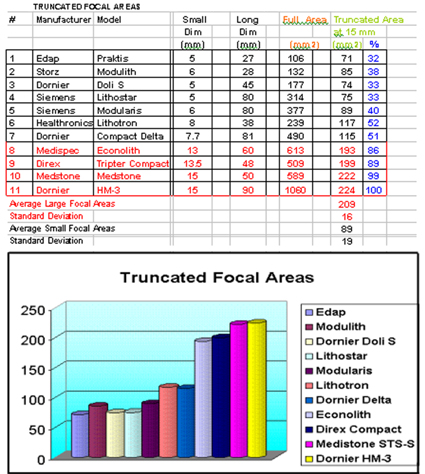
The Peak Pressure at F2 and the Focal Area are the traditional parameters used to compare the performance and effectiveness of the Shock Wave produced by different lithotripters. Lately, new electromagnetic lithotripters were introduced, some with higher Focal Peak Pressure. This fact may lead to believe that they are more efficient than the traditional spark gap systems. At the same time all electromagnetic systems have very thin focal areas, much smaller than the typical stone size, and therefore the available energy is not optimized for stone fragmentation, usually requiring much more shocks compared to a traditional Electrohydraulic lithotripter. The Focal Cross Section at F2, the Truncated Focal Area and Volume are 3 new tools which allow a more accurate evaluation of the Shock Wave characteristics and efficiency of different lithotripters. Eleven currently used lithotripters including the Dornier HM-3 were compared: The results show two categories of Lithotripters: a) Large Focus: Dornier HM-3, Medstone STS-T, Direx Tripter Compact and Medispec Econolith. b) Small Focus: All electromagnetic lithotripters, plus Edap Praktis and the Healthronics Lithotron. The Average Focal Cross Section for Large Focus lithotripters is 5 times bigger than the small ones. The Average Truncated Area is 2.35 times bigger and the Average Truncated Volume is 5 times bigger in Big Focus Lithotripters compared to Small Focus ones. This may help to explain why usually the electromagnetic lithotripters require much more shocks to break stones and have larger retreatment rates. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| INTRODUCTION | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Various lithotripters using different Shock Wave technologies are currently offered to treat stones in the urinary tract. In order to compare the various systems offered, Urologists analyze their technical specifications to evaluate their performance. (Ref 1) Traditionally the Peak Bar Pressure at F2 is the first parameter considered as an indicator of the available energy of a lithotripter and, therefore, has served as a first indicator of the efficiency of the system. Some confusion existed in the past regarding the numerical value of this Pressure at F2. Due to specific conditions of the Shock Waves, the measurements done with the older Piezoelectric Crystal sensors lead to erroneous high values of pressure (above thousand bars). During the last years a new precise sensor made of a membrane of Poly Vinyl Duo Fluoride (PVDF) was developed and adopted by FDA as the only one to be used in Pressure measurements (Ref 2). Using PVDF, the pressure values recorded are "smaller" compared to old Piezoelectric Crystal sensors, but obviously this is are more accurate and "real" values. Recently, new Electromagnetic lithotripters were introduced some of them with higher Peak Bar Pressure. This fact leads one to believe that they are more efficient than the traditional spark gap systems. Looking carefully we can see that this may be misleading. A correct analysis requires one to look not only at the Peak Bar pressure but also at the focal area geometric dimensions. All Electromagnetic systems have very thin focal areas - much smaller than the typical stone size-and, therefore the available energy is not optimized for stone fragmentation. The Total Focal Area which is also used sometimes to compare different lithotripters may be misleading too, because it does not take into account the fact that the typical stone size is much smaller than the long axis of the Focal ellipse and therefore a big portion of the energy is not applied to the stone. In order to clarify this issue three new tools were developed and are presented: b) The Truncated Ellipse Focal Area c) The Truncated Focal Volume. They will allow a more precise geometrical comparison of the Focal Areas of different lithotripters and hence their effectiveness. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MATERIALS AND METHODS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
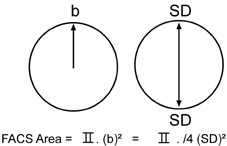
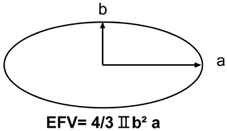
1) Focal Area Cross Section (FACS) The easiest way of visualizing how much of the stone is subjected to pressure is to look at the Cross Section of the ellipsoid at F2 (Like "cutting" the ellipsoid/cigar at F2 and looking at the circle that originated).
b = Focal Short Radius =SD/2 2) Ellipse shape geometric function 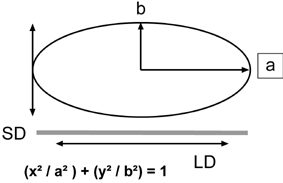
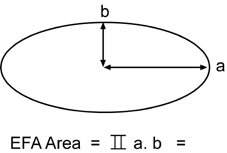
Using the ellipse Long Radius a , and the Short Radius b, we can calculate the full Ellipse area using the formula
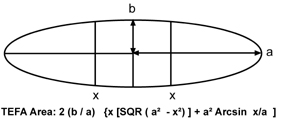
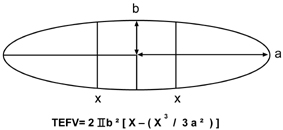
4) Truncated Ellipse Focal Area (TEFA)
RESULTS
2) The Truncated Ellipse Focal Area The Graph below represents all focal ellipses and their truncation.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| DISCUSSION | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This may explain why the electromagnetic devices typically require significantly more shocks to adequately fragment kidney stones and also may result in higher retreatment rates. Recently, concerns have been raised ( Ref 5) regarding the fact that some new Electromagnetic Lithotripters that have very small focal areas and extremely high peak positive pressures are reporting higher clinically significant hematoma rates of 3 to 12% (Ref 6,7 and 8). A trend that is worrisome. It is becoming clear that the electromagnetic devices with very long and thin focal area/volumes are not suited to fragment stones. The Truncated Areas and Volumes are intended to advance the discussion relative to the effectiveness of various lithotripters. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| REFERENCES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. J. Stuart Wolf, Jr. M.D. Issues in choosing a Lithotriptor: Concepts in Design and use. AUA, 2001. 2. Lewin P.A. and Schafer M.E. "Shock Wave sensors: Requirements and Design. J. Lithotripsy and Stone Disease vol. 3 pp 3-17, 1991. 3. IEC International Standard pressure Pulse Lithotripters-Characteristics of Fields. 1998 -04 Annex C, page 21. 4. FDA Guidance for the Content of Premarket Notifications (510 k) for Extracorporeal Shock Wave Lithotripters Indicated for the Fragmentation of Kidney and Ureteral Calculi. August 9, 2000. Page 6. 5. 1st International Consultation on Stone Disease Committee 8: Bioeffects and Physical Mechanisms of SW Effects in SWL. Chairman: James E. Lingeman, M.D. et al. 6. Kohrmann KU, Rassweiler JJ, Manning M, et al. The clinical introduction of a third generation lithotriptor Modulith SL 20. Journal of Urology, 1995; 153:1379-1383. 7. Stefan T, Thorsten B, Chaussy C. Reduced retreatment rate by anatomy related shockwave (SW) energy. Journal of Urology, 1998; 159:S34 (abstract). 8. Piper NY, Dalrymple N, Bishoff JT. Incidence of renal hematoma formation after ESWL using the new Dornier Doli-S lithotriptor. Journal of Urology, 2001; 165:S377 (abstract). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
SUBMITTER ADDRESS LISTING FOR CDRH SUBSTANTIALLY EQUIVALENT (SE) 510(K) SUMMARIES OR 510(K) STATEMENTS FOR FINAL DECISIONS RENDERED DURING THE PERIOD 01-JAN-2003 THROUGH 31-JAN-2003 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1) Introduction A .." Unfortunately current lithotriptor designs have not been based on fundamental advances in the basic science of SWL vis-?-vis stone comminution and tissue effects. The result has been that newer generation machines have not improved outcomes for patients and indeed may be both less effective in breaking stones and more traumatic to renal tissue. "
2) Page 9 3) Page 10 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
100 treated cases with NOVA ULTIMA Extra Corporal Lithotripter Dr. Ruben Munoz, Dr. Pierre P. Tirolien |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
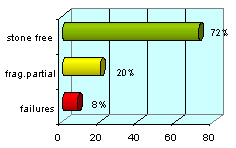
The lateral posture permits an excellent ultrasound scans image avoiding abdominal and suprarenal folds and also an improvement to the skin contact with the membrane. Results: The results in a three months period had been:
The best results obtained were with the pelvic and lumbar urethral stones (82%)
Discussion: For the kidney and urethral stones treatment on obese patients the lithotripter features are very important and the operator experience too. The knowledge and application of the localization systems permits to the specialist to obtain a better percentage of stone free. These techniques are important for these patients due to the posture on the table, which is fundamental to obtain a good result (50% in lateral posture with ultrasound scan). Conclusion: The indication of using ESWL on obese patients is a good choice but we always have to be respectful with the criteria of selection. The percentage of stone free in a three-month period has been satisfactory and the complications are similar to the ones published by other authors.
XIV National Conference of Lithiasis and Urinary Endoscopy,
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||





Suit actor was a white face new version, please wear a blue stripe red replica watches sale drive, white and classic Le Mans 1970 film excellent. The Porsche 917 Gulf driving scenes of his, in tag heuer replica uk real estate department insisted on giving Joe Siffert including a driving replica tag heuer watches chronograph suits overall also natural to him. Always, 24 hours, Heuer representatives of many set up by rolex replica uk that has been proud to wear the watch company logo and officially in rolex replica sale rally champion and rider, Switzerland Joe Siffert, is famous it was the first of. Of course, Steve Monaco dressed in his wrist has contributed to its popularity. The replica watches sale style, ultra-modern of them, becomes one of the deviation complete popular replica watches among the artwork traditional, however, it is not the only reason.